Cervical spondylomyelopathy – exploring the diagnosis and complexities of wobbler disease
By Professor Noel Fitzpatrick
1. What makes cervical spondylomyelopathy a challenging diagnosis?
Cervical spondylomyelopathy (CSM), often referred to as ‘wobbler disease’, is a multifactorial condition affecting the cervical spine in larger breed dogs – resulting in progressive compression of the spinal cord and nerve roots. Morphologic and biomechanical abnormalities of the cervical spine have been classified as either Disc-Associated Wobbler Syndrome (DAWS) or Osseous Associated Wobbler Syndrome (OAWS).
Dobermans are predisposed to DAWS, but the disease can also occur in breeds such as Labradors and Dalmatians. Great Danes and Basset Hounds can be predisposed to OAWS. DAWS involves protrusion of one or more degenerative cervical discs into the spinal canal, usually affecting C5-6 and C6-7, causing compression of the spinal cord or nerve roots. In OAWS the spinal cord is compressed as a result of malformation and proliferation of the osseous boundaries of the spinal canal (facets and neural arch). In both presentations, the spinal cord can be compressed chronically without major symptoms and then a minor incident can trigger deterioration, manifested as cervical pain (nerve root compression) or ataxia (spinal cord compression), which can progress to para or tetra-paresis / plegia.
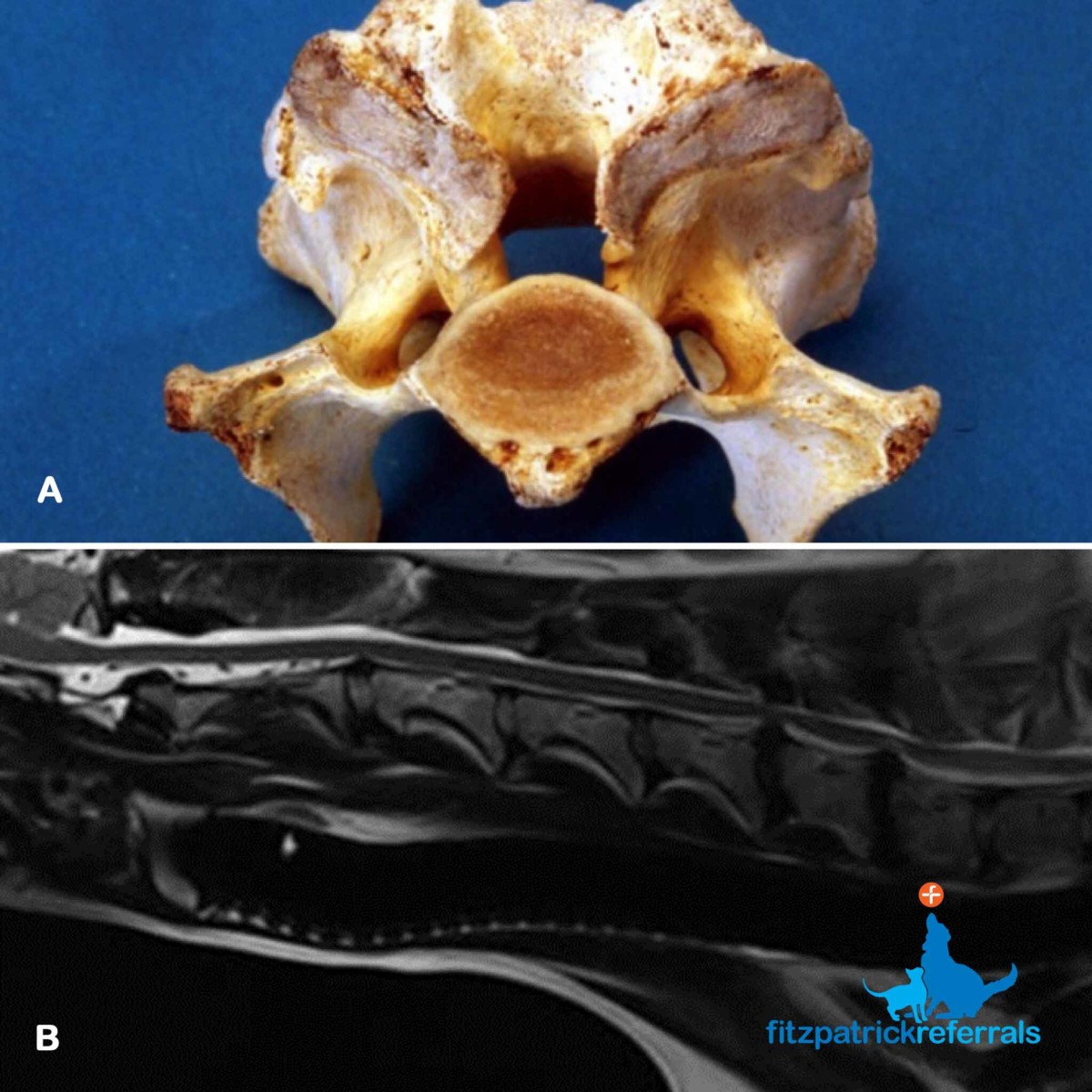
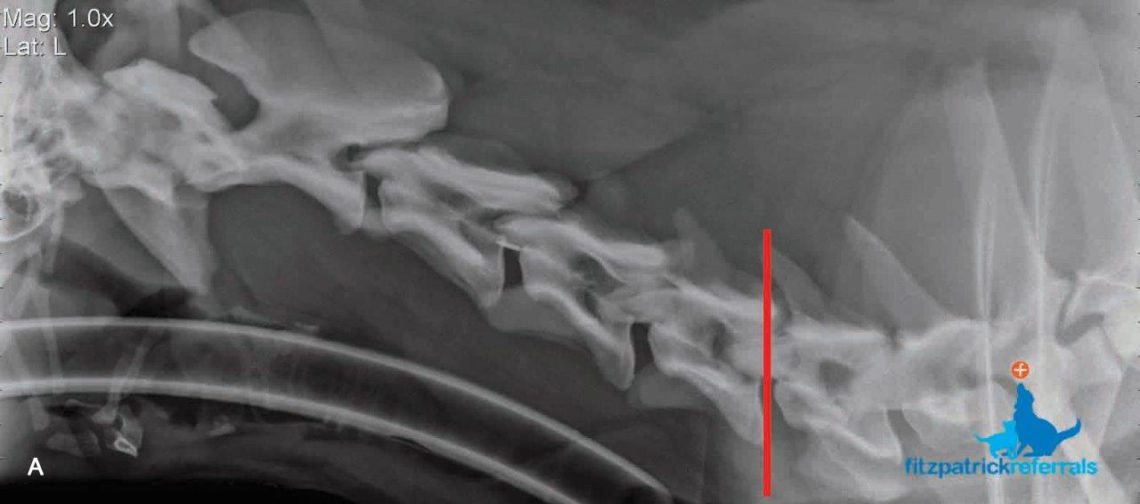
(A) A post-mortem sample of a vertebra affected by osseous compression of the spinal canal (OAWS). (B) Sagittal plane T2-weighted MRI scan of intervertebral disc protrusions at C5-6 and C6-7 (DAWS).
2. Why is advanced imaging crucial for an accurate diagnosis?
Survey radiography is not sufficient for the diagnosis of either DAWS or OAWS. MRI scans are considered fundamental to elucidate the degree of spinal cord impingement. Dynamic MRI imaging can be performed to investigate if a disc protrusion causes more compression in extension (dynamic) or if the degree of compression reduces when traction is applied to the neck (traction-responsive). A high-powered scanner which allows variable positioning is essential. CT scans optimally illustrate osseous margins and are important for measurement if surgery using implants is planned.
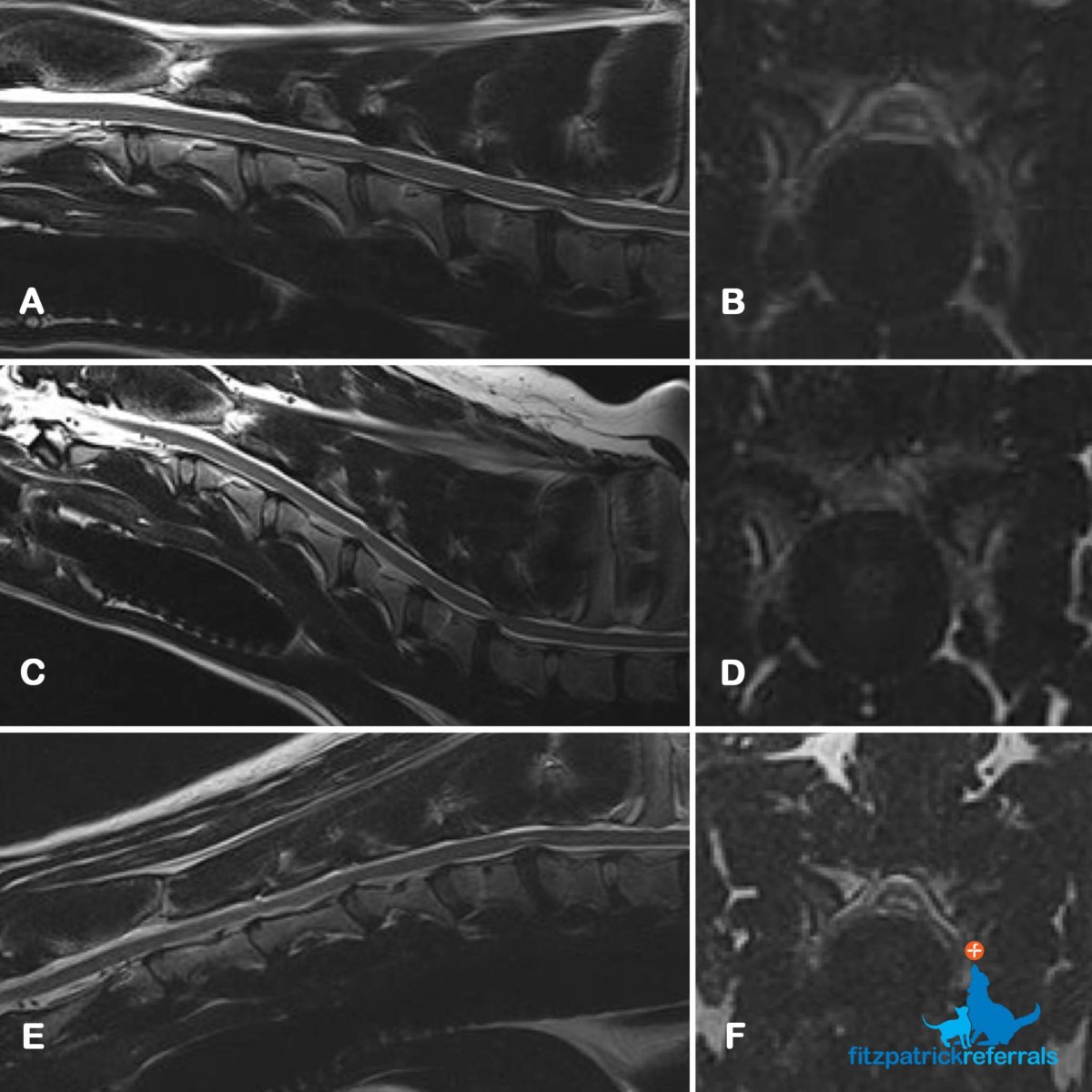
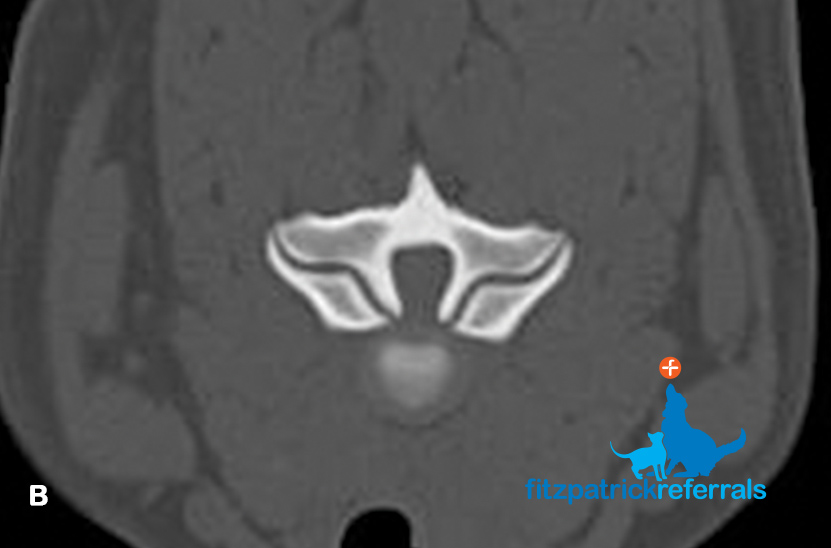
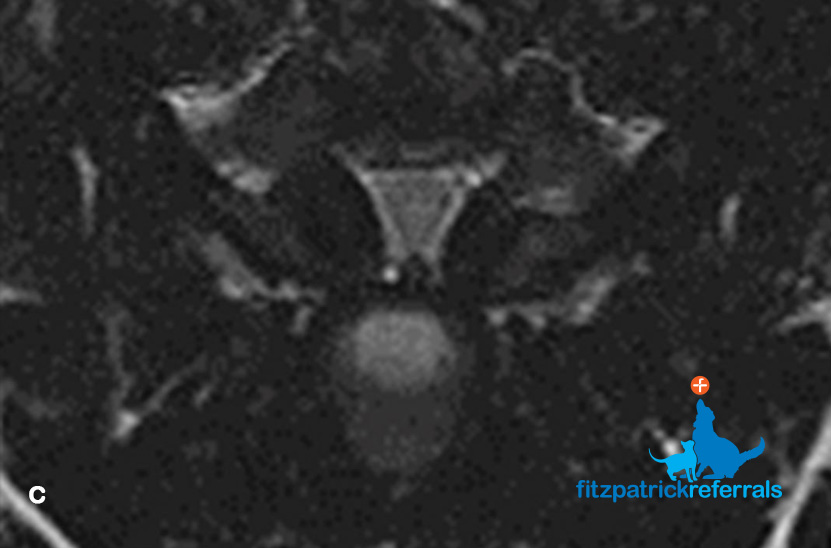
Images A-F are T2-weighted MRI sagittal and transverse images of a C6-7 intervertebral disc protrusion in a five-year-old Doberman affected by DAWS illustrating three different positions.
A,B Neutral; B,C Hyperextended; E, F Traction.
The spinal cord is more compressed in hyperextension and less compressed when traction is applied. Note the increased signal intensity within the cord due to vasogenic oedema, gliosis and/or malacia. This may not resolve even after surgical treatment.



3. What treatment options are available?
Historically, many techniques have been evolved in an effort to achieve distraction of the disc space and alleviate compression in DAWS cases, with variable success. Dorsal laminectomy or facetectomy have been typical surgical interventions for OAWS patients. This can be successful, especially for single or double lesions requiring limited bone removal, but high morbidity has sometimes been experienced with extensive multiple site decompression and it can be difficult to remove bone from the neuroforaminae with a dorsal decompression.
We have developed and published outcome measures on a distraction-fusion system for both DAWS and OAWS patients that we have employed with considerable success for many years. This technique is unique to Fitzpatrick Referrals and involves distraction through insertion of a conical threaded spacer (Fitz Intervertebral Traction Screw, FITS) and a linkage system of plates and rods (‘Fitzateur’) which is custom made for each patient with exactly correct vertebral screw positioning.
The fusion devices can be deployed for single or multiple sites, and in conjunction with application of bone graft, promotes permanent fusion of the vertebrae. We have proven that both osseous and soft tissue compressive elements of the spinal cord and nerve roots can regress over time and that clinical improvement can be robust and resilient.
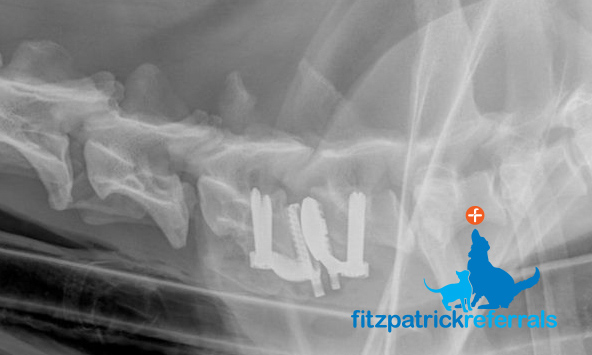
A radiograph of a custom-made Fitz-Disc – alleviating compression caused by disc protrusion between adjacent vertebrae whilst maintaining motion.
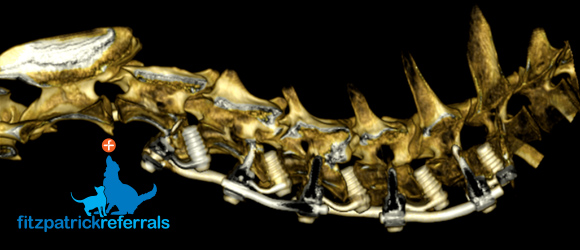
A 3D rendered CT scan of a FITS-Fitzateur device employed for multiple site distraction-fusion in DAWS or OAWS cases – providing immediate and resilient decompression of the spinal cord and nerve roots.
With some DAWS patients, it may be advantageous to maintain motion at the affected site since fusion may result in stress concentration into adjacent sites, potentially predisposing to ‘adjacent segment disease’ or ‘domino effect’ whereby disc disease may manifest more readily at locations cranial or caudal to the fused site. At Fitzpatrick Referrals, we have developed and proved efficacy for a custom-made disc replacement (‘Fitz-Disc’) which spaces the vertebrae, maintains motion and is secured to the bone with screws to prevent loosening.

{kind=link}
{kind=link}
{kind=link}