What is total knee replacement?
Total knee replacement (TKR) involves removing the articulating parts of the diseased knee joint and replacing the joint surfaces with a prosthetic joint; this surgery is very similar to the one performed in humans.
How can I tell if my dog would benefit from a total knee replacement?
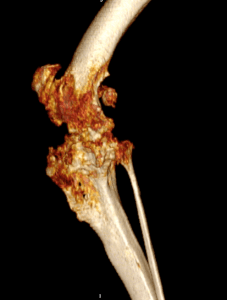
Total joint replacement of any joint carries the risks of possible complications. Therefore, total knee replacement is reserved for dogs with painful knee conditions, where either conventional surgical techniques have not been successful or where diseased joints are unresponsive to conservative management using pain relief and rehabilitation. The most common cause of knee pain is osteoarthritis secondary to cruciate disease, trauma or malformation of the knee. Examples of severe osteoarthritis are shown below:


The primary goal of total knee replacement surgery is to restore pain-free function of the knee. In most cases, it is possible to restore joint function to a level that is similar to a healthy knee. Dogs that have had successful TKR surgery usually do not require long-term medical management with pain medication.
What types of total knee replacement are available?
Fitzpatrick Referrals offers two distinct total knee replacement systems: a commercial system and a custom-made system which is individually designed for each dog.
Commercial BioMedtrix total knee replacement
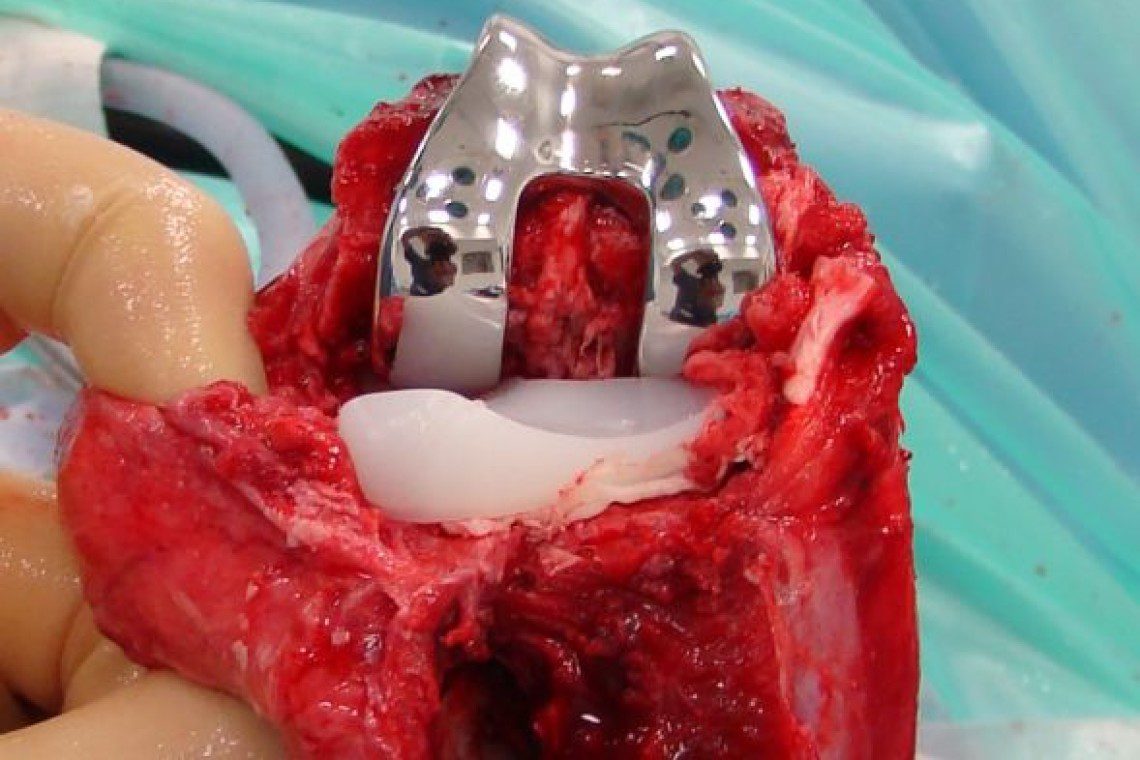
The commercial system consists of a polyethylene (plastic) component that is fixed to the tibia and a metal component that is fixed to the femur. The two components articulate with each other, creating a new weight-bearing surface and mimicking the movement of a normal joint during knee motion. The commercial total knee replacement system is suitable for dogs >15kg body weight. It is, however, reliant on the stabilising ligaments of the knee joint, known as the collateral ligaments – on the outside and inside of the knee – being intact for your dog to be suitable for a commercial total knee replacement; the cruciate ligaments do not need to be.


Custom-made total knee replacement
Fitzpatrick Referrals offers custom-made total knee replacements for cats, small dogs and dogs with either severe traumatic knee injury or severe degenerative knee disease; these pathologies often result in damage of stabilising ligaments, therefore increasing knee instability and would make the dogs unsuitable for commercial total knee replacement.
Fitzpatrick Referrals is the only centre in the UK to have pioneered a custom-made, total knee replacement that can be designed for the individual dog’s size and bone anatomy. It is based on a hinged design, featuring more inherent stability compared to the commercial total knee replacement and hence is not reliant on the stabilising ligaments of the knee.
The first step to get your dog’s custom-made total knee replacement implant is to perform a detailed 3D image of your dog’s knee using a CT scanner, which is performed by our advanced diagnostic imaging team while your dog is under heavy sedation or a short general anaesthesia. Our medical engineers then use the 3D CT image to design an implant that exactly fits the dimensions of your dog’s knee. Once the design process is complete, the implant is manufactured using a 3D printing process known as laser sintering, which allows creation of intricate metal implants in the shape of the knee joint that requires replacement. Once your dog’s implant has been manufactured, surgery can be scheduled.

What does total knee replacement surgery involve?
During surgery, the stifle joint (knee) is exposed through an incision on the side of the knee. The joint surfaces of both the femur and tibia are removed and replaced by two components. In the commercial system, a metal component is used to replace the damaged joint surface of the femur and an ultra-high molecular weight polyethylene (UHMWPE, plastic) implant is used to replace the damaged joint surface of the tibia; both components are fixed using orthopaedic cement. As the success of the commercial surgical system relies on the supporting ligaments of the knee, these ligaments are thoroughly checked prior to completion of the surgery.
When your dog gets a custom-made total knee replacement, both components are made of metal.
What are the risks of total knee replacement?
The most significant risks associated with total knee replacement surgery are infection of the implants, infection of the joint, implant loosening and failure of the supporting ligamentous structures. Infection is a rare but potentially devastating complication of this surgery, as it is for any other orthopaedic procedure; the risk of loosening is also rare. In both complications, implants might need to be explanted to get on top of the infection or to remove the loose component. To prevent damage to the supporting ligaments, which can occur due to the changed biomechanical load and strain on the ligaments when the commercial system is used, careful postoperative management of the dog and rehabilitation of the knee is beneficial.
What is the typical recovery time after total knee replacement?
Recovery to return to normal exercise lasts about 12 weeks after surgery and is assisted by a structured post-operative rehabilitation programme, which is created by our physiotherapy team in collaboration with the operating surgeon. Careful rehabilitation after total knee replacement is the key to success.
During your dog’s hospitalisation with us, he/she will be cared for by a dedicated patient care team who work alongside your dog’s clinician, a team of veterinary surgeons and chartered physiotherapists, who ensure that your dog’s clinical and emotional needs are met. As your dog will remain hospitalised for a number of days following surgery, our patient care team will make sure they feel at home and are treated with the love and affection your dog desires and deserves.
It is vital that dogs who undergo total knee replacement surgery are managed diligently for the first 7-10 days after surgery to prevent damage to the operated knee. In the postoperative period at home, dogs will follow a carefully managed exercise programme that gradually brings them back to off-lead exercise by 12 weeks after surgery.
How long will the total knee replacement implant last?
For the commercially available BioMedtrix, excellent clinical function over the course of at least 6 years with good implant position and fusion of the implant with the bone has been published in a peer-reviewed case report in 2025. Unfortunately, to date, there are no studies published looking at the long-term performance of this TKR implant in a larger population of dogs.
For the custom rotating hinge TKR implant, we have subjective data from our hospital for dogs that have been living with their implants without any problems for up to 5 years. Unfortunately, we do not have any data after 5 years, as the implant is quite new. Therefore, we don’t have enough data yet to provide a definitive answer to this question for either the commercial or the custom TKR implant.
In people, total knee replacement implants are expected to last more than 15 years. Implant survival depends on the long-term stability of the implant, maintenance of a smooth articulation between the components, and the patient’s activity level. We expect that the implants will survive the lifetime of a dog.
Are there reasons why my dog shouldn’t have total knee replacement surgery?
If your dog’s knee pain is effectively controlled with pain medication and rehabilitation, it is unlikely that joint replacement surgery would be recommended for your dog.
There are also absolute contraindications – situations when a total knee replacement should not be performed. These include: septic arthritis (infection of the knee), osteomyelitis (infection of the bone), systemic infection, certain neurological conditions like peripheral nerve paralysis (the muscle-nerve connection does not work and limb movement is difficult) or spinal cord disease. Other conditions that significantly affect mobility, such as painful hip dysplasia, may also preclude surgery.
If your dog is in poor general health, has a hormone-related disease, is immunosuppressed, has poor bone quality or suffers from severe obesity – this can influence the decision-making for or against a total knee replacement. It is also worth noting that dogs will need to be confined and restricted in their exercise regime for several weeks after surgery to have a chance of a successful outcome, which might be difficult in some dogs and which makes client compliance of utmost importance.
What alternatives to total knee replacement are available?
Arthrodesis, or fusion of the knee joint, may be a viable alternative in dogs that are not suitable candidates for total knee replacement. However, function of a fused knee is particularly sub-optimal in comparison to total knee replacement.
What should I do if I think my dog needs a total knee replacement?
If you think your dog needs a total knee replacement, we recommend asking your primary care vet to contact us for further advice. We are more than happy to talk to your vet about what is involved with the surgery and ascertain if total knee replacement would be an option for your dog.
Patient story
Lucy | Custom hinged total knee replacement
Lucy is a 10-year-old golden retriever who was referred with significant pain and lameness affecting her left hind limb, attributed to considerable arthrosis of the knee. A CT scan revealed collapse of the medial compartment (one half of the knee) with bone-on-bone wear and complete erosion of the caudo-medial tibial plateau (parts of the tibia articular surface). In Lucy’s case, the cruciate and collateral ligaments were disrupted. Therefore, a custom rotating-hinge total knee replacement was designed and manufactured for her. The two components had one metal stem each that were anchored into the femur and tibia using cement, while hydroxyapatite cover on metal surfaces that had direct contact with bone helped with bone on-growth.
Six months postoperatively, Lucy’s lameness has completely resolved and she enjoys unrestricted activity.